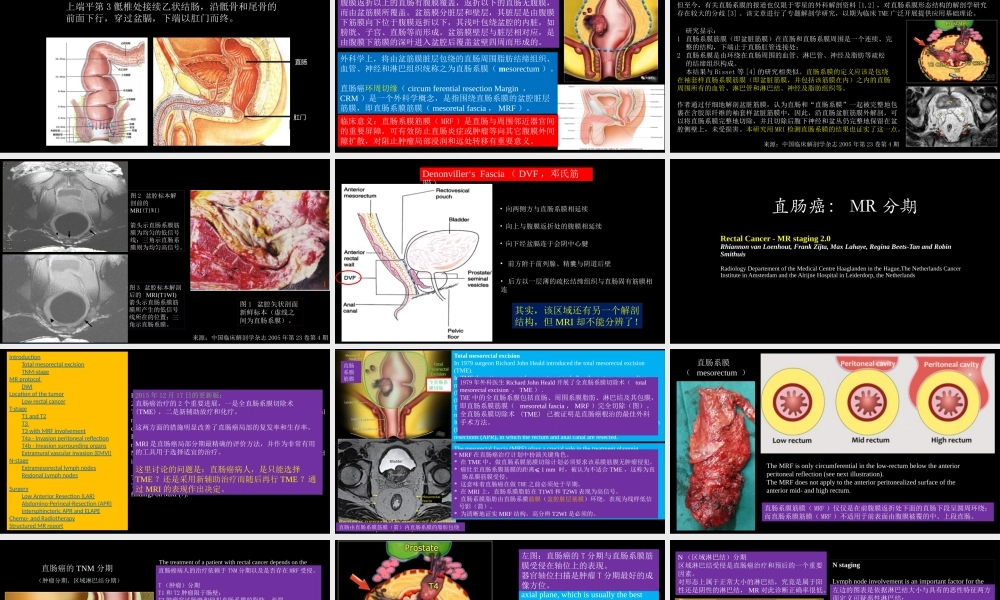
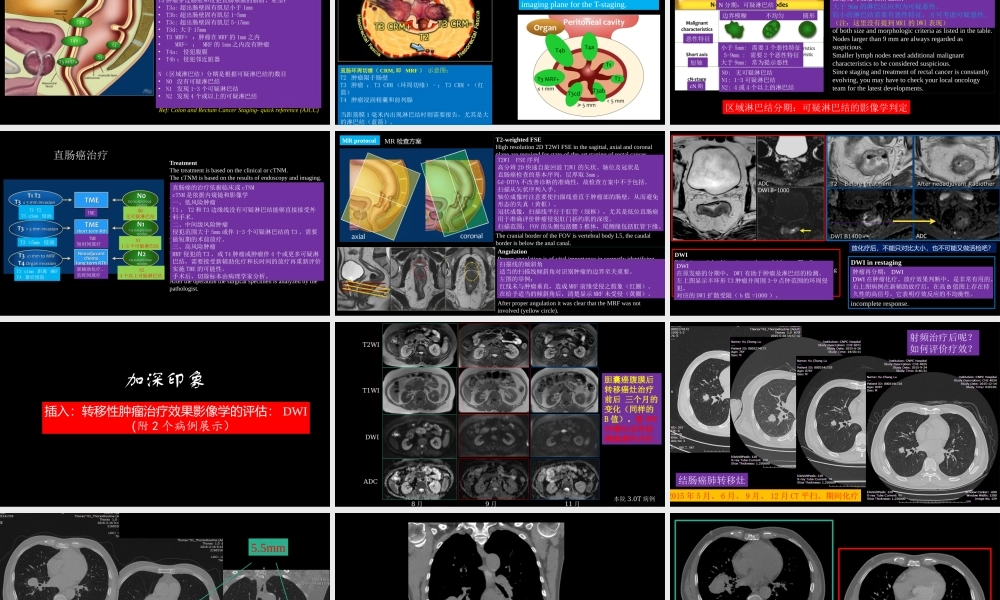
杨景震编译制作直肠癌:MRI与临床(内有动画设计,浏览请用放映模式)直肠为大肠的末段,长约15-16cm,位于小骨盆内。上端平第3骶椎处接续乙状结肠,沿骶骨和尾骨的前面下行,穿过盆膈,下端以肛门而终。直肠肛门外科学上,将由盆筋膜脏层包绕的直肠周围脂肪结缔组织、血管、神经和淋巴组织统称之为直肠系膜(mesorectum)。直肠癌环周切缘(circumferentialresectionMargin,CRM)是一个外科学概念,是指围绕直肠系膜的盆腔脏层筋膜,即直肠系膜筋膜(mesoretalfascia,MRF)。相关基本概念全直肠系膜切除术(totalmesorectalexcisionTME)解剖学基础:腹膜返折以上的直肠有腹膜覆盖,返折以下的直肠无腹膜,而由盆筋膜所覆盖。盆筋膜分脏层和壁层,其脏层是由腹膜下筋膜向下位于腹膜返折以下,其浅叶包绕盆腔的内脏,如膀胱、子宫、直肠等而形成。盆筋膜壁层与脏层相对应,是由腹膜下筋膜的深叶进入盆腔后覆盖盆壁四周而形成的。临床意义:直肠系膜筋膜(MRF)是直肠与周围邻近器官间的重要屏障,可有效防止直肠炎症或肿瘤等向其它腹膜外间隙扩散,对阻止肿瘤局部浸润和远处转移有重要意义。来源:中国临床解剖学杂志2005年第23卷第4期明确直肠系膜的解剖学结构是应用全直肠系膜切除术(totalmesorectalexcision,TME)治疗直肠癌的基础。但至今,有关直肠系膜的报道也仅限于零星的外科解剖资料[1,2],对直肠系膜形态结构的解剖学研究存在较大的分歧[3]。该文章进行了专题解剖学研究,以期为临床TME广泛开展提供应用基础理论。研究显示:1直肠系膜筋膜(即盆脏筋膜)在直肠和直肠系膜周围是一个连续、完整的结构,下端止于直肠肛管连接处;2直肠系膜是由环绕在直肠周围的血管、淋巴管、神经及脂肪等疏松的结缔组织构成。本结果与Bisset等[4]的研究相类似。直肠系膜的定义应该是包绕在袖套样直肠系膜筋膜(即盆脏筋膜,并包括该筋膜在内)之内的直肠周围所有的血管、淋巴管和淋巴结、神经及脂肪组织等。作者通过仔细地解剖盆脏筋膜,认为直肠和“直肠系膜”一起被完整地包裹在含胶原纤维的袖套样盆脏筋膜中,因此,沿直肠盆脏筋膜外解剖,可以将直肠系膜完整地切除,并且切除后腹下神经和盆丛仍完整地保留在盆腔侧壁上,未受损害。本研究用MRI检测直肠系膜的结果也证实了这一点。解剖学研究与MRI影像图2盆腔标本解剖前的MRI(T1WI)箭头示直肠系膜筋膜为均匀的低信号线;三角示直肠系膜则为均匀高信号。图3盆腔标本解剖后的MRI(T1WI)箭头示直肠系膜筋膜...