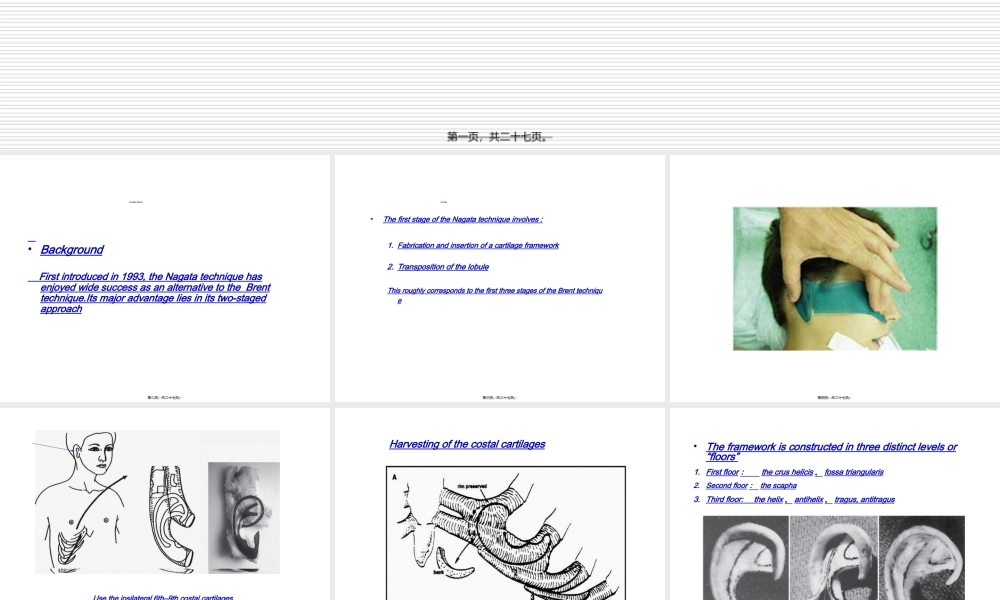
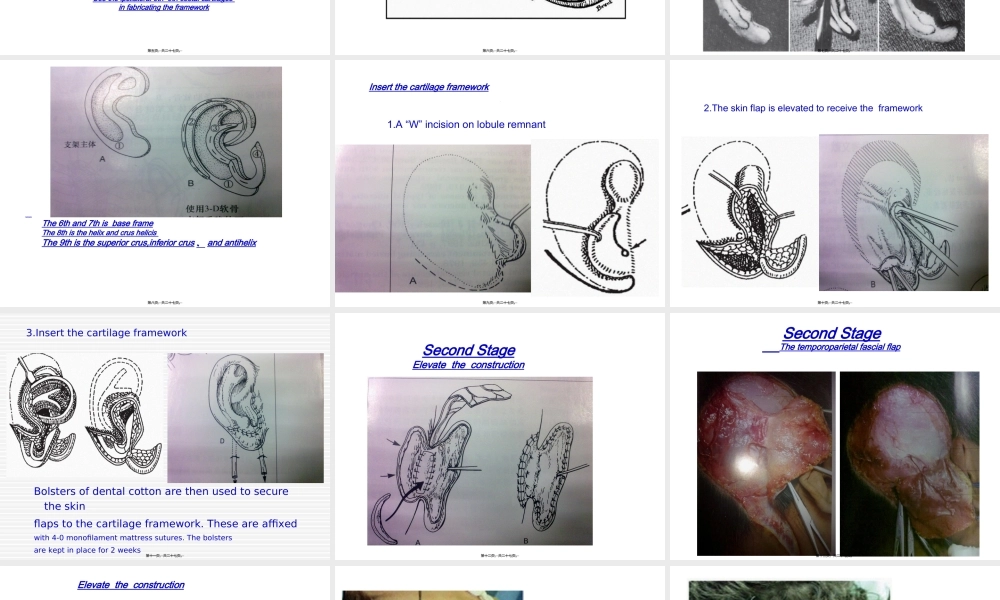
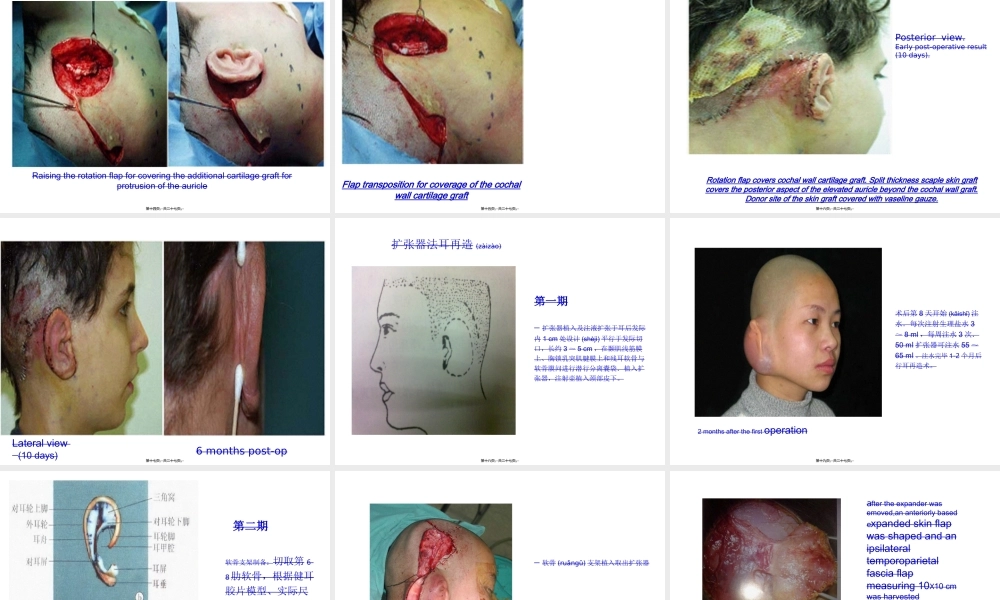
小耳畸形(jīxíng)第一页,共二十七页。TheNagataTechnique•BackgroundFirstintroducedin1993,theNagatatechniquehasenjoyedwidesuccessasanalternativetotheBrenttechnique.Itsmajoradvantageliesinitstwo-stagedapproach第二页,共二十七页。•ThefirststageoftheNagatatechniqueinvolves:1.Fabricationandinsertionofacartilageframework2.TranspositionofthelobuleThisroughlycorrespondstothefirstthreestagesoftheBrenttechniqueFirstStage第三页,共二十七页。第四页,共二十七页。Usetheipsilateral6th–9thcostalcartilagesinfabricatingtheframework第五页,共二十七页。Harvestingofthecostalcartilages第六页,共二十七页。•Theframeworkisconstructedinthreedistinctlevelsor“floors”1.Firstfloor:thecrushelicis、fossatriangularis2.Secondfloor:thescapha3.Thirdfloor:thehelix、antihelix、tragus,antitragus第七页,共二十七页。FabricationThe6thand7thisbaseframeThe8thisthehelixandcrushelicisThe9thisthesuperiorcrus,inferiorcrus、andantihelix第八页,共二十七页。Insertthecartilageframework1.A“W”incisiononlobuleremnant第九页,共二十七页。2.Theskinflapiselevatedtoreceivetheframework第十页,共二十七页。Bolstersofdentalcottonarethenusedtosecuretheskinflapstothecartilageframework.Theseareaffixedwith4-0monofilamentmattresssutures.Thebolstersarekeptinplacefor2weeks3.Insertthecartilageframework第十一页,共二十七页。SecondStageElevatetheconstruction第十二页,共二十七页。SecondStageThetemporoparietalfascialflap第十三页,共二十七页。ElevatetheconstructionRaisingtherotationflapforcoveringtheadditionalcartilagegraftforprotrusionoftheauricle第十四页,共二十七页。Flaptranspositionforcoverageofthecochalwallcartilagegraft第十五页,共二十七页。Rotationflapcoverscochalwallcartilagegraft.Splitthicknessscapleskingraftcoverstheposterioraspectoftheelevatedauriclebeyondthecochalwallgraft.Donorsiteoftheskingraftcoveredwithvaselinegauze.Posteriorview.Earlypost-operativeresult(10days).第十六页,共二十七页。Lateralview(10days)6monthspost-op第十七页,共二十七页。扩张器植入及注液扩张于耳后发际内1cm处设计(shèjì)平行于发际切口,长约3~5c...